












Problems With CDC Studies Allegedly Proving Masks Are Effective
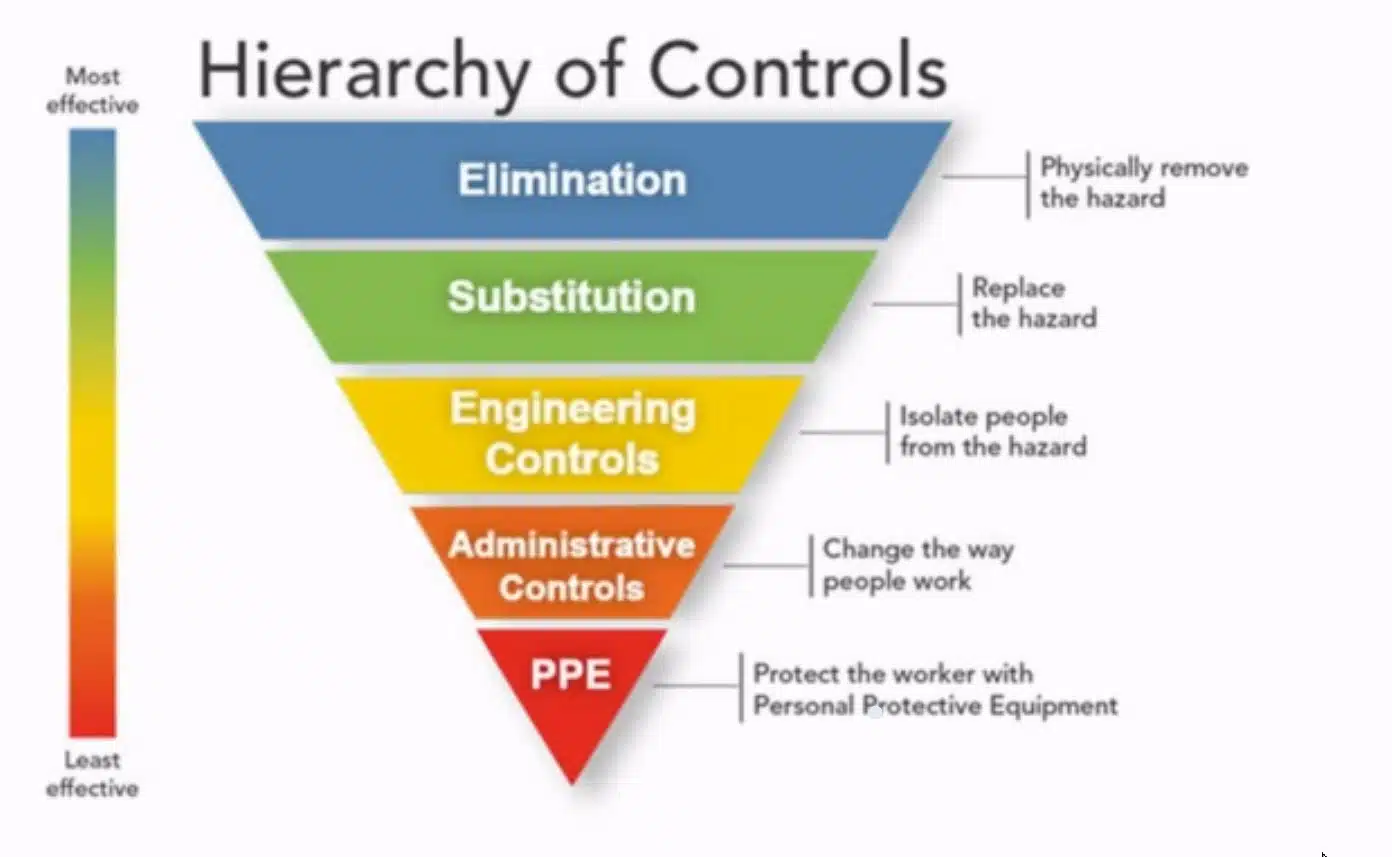
Look at that pyramid infographic above. Most of the studies set forth by the CDC and others who claim that universal masking – or using a mask at all – will work to protect people from spreading Covid-19 or being infected by it, didn’t even make it out of the Level 4 – “Starting Points”.
Some made it to Level 3. This is especially true with the CDC’s studies in support of mask mandates. Ignoring these critical steps is dangerous to the public. The CDC ignored the most important steps in their public policy formulation.
Doctors don’t use masks to protect themselves from being infected. The purpose for which health professionals use masks is to protect the patient from the Doctor sneezing or coughing droplets into an open wound or onto a patient.
Surgical masks have nothing to do with protection against aerosols. Medical settings (hospitals) and laboratory testing facilities have a number of other infection mitigations happening at the same time as wearing masks.
Testing in these environments produces skewed results.
Some examples of other mitigations to filter out virus particles are: HVAC systems, negative or positive pressure rooms with no air flow in or out of the room and PPE with specific donning and doffing routines applied by trained professionals.
These procedures are the result of Exposure Science. They were developed by scientists and engineers of the exposure science field over many decades of experience.
When the CDC posted about 70 studies on their website in the late summer of 2020, allegedly proving that “masks work,” the true believers out there were emboldened to be morally justified when they denigrated non-mask wearers. Amazingly, such public shaming of non-mask-wearers persists to this day (August 25, 2022).
What – Exactly – Happens With Universal Masking of the Public?
The last half of Tyson Gabriel’s video to which I’m referring, deals with the countless flaws in these studies. As I already stated, he points out that each and every study set forth by the CDC to “prove” the efficacy of universal masking, fails to answer one basic question:
“What – exactly – happens with Universal Masking of the Public?”
Nobody at the CDC bothered to ask this question. The CDC used laboratory studies under controlled conditions. Here are just some of the flaws Mr. Gabriel found:
- Test subjects held their breath
- In some, they breathed only through their nose
- People held their head in a steady position
- They used old equipment which was not calibrated (this was admitted in one preprint, omitted in a new preprint)
- Nearly every study made a point to comment on a discovery which made it sound as if it was of great importance. But these were not new discoveries. They were well-known to exposure scientists
- What happens when masks are worn for hours on end in the real-world?
- What happens when mask is cross-contaminated?
- What happens when masks are worn daily for weeks and weeks?
- When eating, the mask is touched, removed, moved to chin, falls to the floor, put in a pocket, on a car seat, re-used multiple times a day, etc. How does that impact the efficacy?
- What happens to the droplets once they are in the mask?
- What happens to the virus particles once the water droplets evaporate?
- Do infectious particles move from the mask surface to other surfaces?
- Does the mask cause extra build-up of virus material? Or bacteria in nasal passages? In lung pathways? Near our brain?
- Additional risks and collateral issues are not studied in the CDC studies
Studies to answer these questions exist. The CDC just ignored and didn’t acknowledge them.
More Variables The CDC Mask-Wearing Studies Failed To Address
Every human breath contains a certain volume of air. That air has to go somewhere when exhaled and comes from somewhere when inhaled. Masks do not impede this flow of air as you saw in Dr. Noel’s vape video demo above. And if they do impede the flow of air too much, serious problems can arise with oxygen and CO2 levels in the mask-wearer.
Donning & Doffing is the specific procedure of putting on and taking off Personal Protective Equipment (PPE) and clothing. Procedures were created by the Exposure Science industry because science showed decades ago that microscopic infections virus and other particles collect on the outside & inside of masks.
This is why Donning and Doffing procedures exist.
Now we place these collection devices (masks) on our children for hours and days on end. This is dangerous. What are they breathing in? What’s growing on the inside of those masks?
People have a right to believe their CDC is competent, honest and disclosing everything. The CDC failed badly with respect to efficacy of Universal Masking.
Update from August 25, 2022:
Who was leading the charge for universal masking in the United States? Dr. Anthony Fauci.
Last week, we learned he is now retiring. Megyn Kelly, an American conservative journalist and political commentator, published a video rant about him on August 25, 2020. It’s about 19 minutes long.
If truthfulness from our non-elected officials like Dr. Fauci matters to you, I suggest you watch it. Be advised, she is passionate and uses some . . . how shall I say . . . “colorful” language in this rant.
She exposes the massive amount of harm Dr. Fauci foisted on the American public. Rather than provide a review here, I suggest you watch it.
Specific Flawed Studies Used To Allegedly “Prove” Mask Efficacy
- September 2020 – WHO commissioned Lancet study claimed to show effectiveness to reduce transmission 80%.
- Mostly was N95s in a hospital setting
- Strength of the study considered “low”
- Numerous flaws found by experts
- Epidemiologist Peter Jueni (University of Toronto) called the study “essentially useless”
- Proceedings of the National Academy of Sciences (PNAS) study claimed decrease in infections in 3 global hot spots. Didn’t take into account other measures and natural decrease. 40 scientists requested the study be withdrawn it was so flawed.
- BMJ Yale – medRxiv ‘ The Preprint Server for Health Sciences’ did another widely publicized study claiming that counties with mask mandates had lower Covid infection rates. But those counties experienced rapid increases of infections shortly after the study was published so the authors had to withdraw it.
- A widely heralded large scale study in Bangladesh involving 600 villages claimed surgical masks were better than cloth masks and showed a reduction of 0.8% but only in people over age 50. But an examination by statisticians of the same study resulted in this statement: “More broadly, the significant impacts on staff and participant behavior urge caution in interpreting small differences in the study outcomes that depended on survey response.” In other words, the study was so flawed as to be useless due to participant behavior and staff biases between the treatment and control groups.
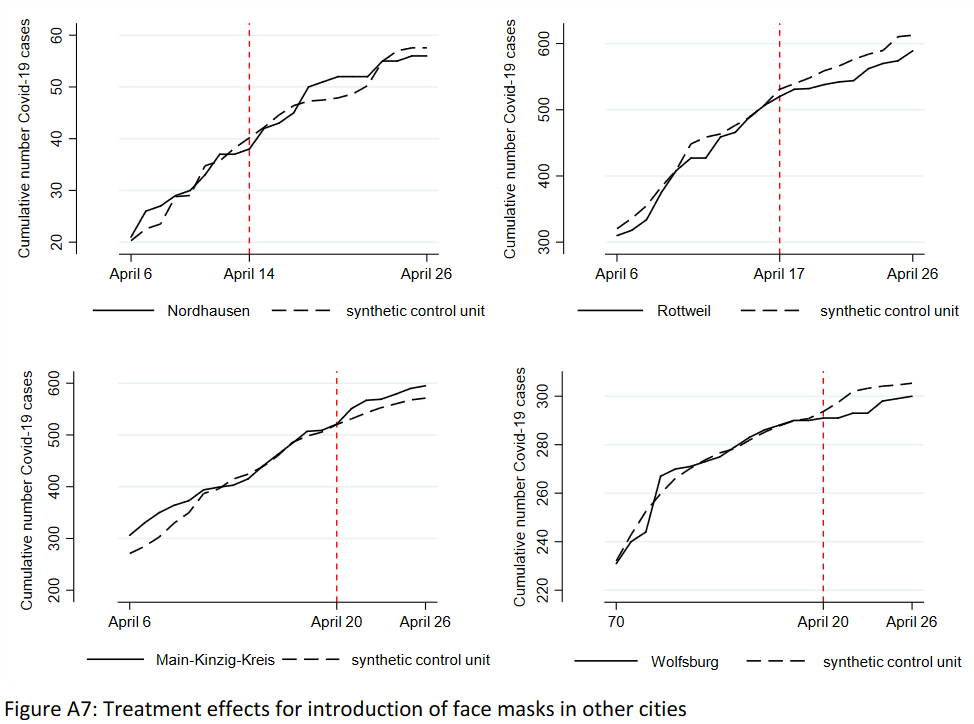
- A German study claiming that mask mandates decreased infections but the data didn’t support the claim. Some cities showed an increase, others showed a decrease and one city, Jena, decreased but only because they simultaneously required strict quarantines, a fact omitted in the study. This study did not show any benefit to mask mandates.
- A University of Oxford review tried to claim face masks are effective. But it was flawed because the study was about SARS-1 and done in health-care settings, not among the community.
- A lobbying group in favor of mask mandates (Masks for All) published in the PNAS journal, claimed that masks block aerosol transmission – but they provided no evidence.
- A study published in Nature Communications in 2021 claimed a 62% reduction of infection by those wearing masks. But this study was merely self-reported survey and modelling, with no actual measurements.
- The BMJ published a study claiming a 53% reduction of infections from wearing masks, but later had to admit in an editorial the “lack of good research” and that the result was implausible.
- Another PNAS study said that N95/FFP2 masks were effective against coronavirus infections, but it was only a model without real world or lab data.
- The CDC ran a study that claimed faced masks reduced Covid infections in schools, but when the study was updated, the effect disappeared.
Inherent Risk Of Using Facemasks For Prolonged Periods
As discovered and reported by the Exposure Science Industry, Universal Masking does more harm than good. Here are just a few examples of harms forced on people during the pandemic:
- WHO published a 22-page detailed PDF in December 2020 encouraging the universal usage of masking up to protect against SARS-CoV-2 transmission and infection. A section of this document warns against the following adverse reactions to the over-use of face masks:
- contamination of the mask due to its manipulation by contaminated hands (53, 54);
- potential self-contamination that can occur if medical masks are not changed when wet, soiled or damaged; or by frequent touching/adjusting when worn for prolonged periods (55);
- possible development of facial skin lesions, irritant dermatitis or worsening acne, when used frequently for long hours (56-58);
- discomfort, facial temperature changes and headaches from mask wearing (44, 59, 60);
- false sense of security leading potentially to reduced adherence to well recognized preventive measures such as physical distancing and hand hygiene; and risk-taking behaviors (61-64);
- difficulty wearing a mask in hot and humid environments
- possible risk of stock depletion due to widespread use in the context of universal masking and targeted continuous mask use and consequent scarcity or unavailability for health workers caring for COVID 19 patients and during health care interactions with non-COVID-19 patients where medical masks or respirators might be required.
- The also admit on Page 8 of this document the following:
“At present there is only limited and inconsistent scientific evidence to support the effectiveness of masking of healthy people in the community to prevent infection with respiratory viruses, including SARS-CoV-2 (75). A large randomized community-based trial in which 4862 healthy participants were divided into a group wearing medical/surgical masks and a control group found no difference in infection with SARS-CoV-2 (76).”
Yet, the WHO, governments worldwide, big tech, mainstream media and social media continued – and still continues – to lecture the general public to “mask up” (. . . or you’ll kill grandma to quote Gabriel Tyson’s video from earlier in this article). - Irritant dermatitis or worsening acknew when used frequently for long hours;
- headache and/or breathing difficulties, depending on type of mask used;
- difficulty with communicating clearly, especially for persons who are deaf or have poor hearing or use lip reading;
- a false sense of security leading to potentially lower adherence to other critical preventive measures such as physical distancing and hand hygiene;
- waste management issues; improper mask disposal leading to increased litter in public places and environmental hazards;
- disadvantages for or difficulty wearing masks, especially for children, developmentally challenged persons, those with mental illness, persons with cognitive impairment, those with asthma or chronic respiratory or breathing problems, those who have had facial trauma or recent oral maxillofacial surgery and those living in hot and humid environments;
- Nature Scientific Reports, bacteria and fungi growing on face masks
- A Canadian-Israeli study from February 2022 shows face masks disrupt holistic processing and face perception in school-aged children.
- Restricted breathing: Here’s video evidence that resulted in policy changes in the State of Oregon, USA, when a runner from Summit HS in Oregon collapses and passes out just as she crossed the finish line in an 800-meter foot race.
- An Italian study showed that face masks and N95/FFP2 masks increased Co2 levels from inhaled air above the acceptable exposure threshold.
- The University of Muenster in Germany discovered SARS-CoV-2 can remain infectious for several days right on the N95 masks and increase the risk of self-infection.
- Several children in China fainted and died after being required to wear a face mask during gym class. The autopsies showed sudden cardiac arrest as the likely cause of death.
- A driver in New Jersey passed out while driving and crashed their car due to wearing an N95 mask behind the wheel. Medical authorities claimed the driver experienced a lack of oxygen and breathed excessive carbon dioxide thanks to the mask.
Conclusion
There’s simply no rational reason for wearing facemasks for the purpose of either protecting one’s self from infection from SARS-CoV-2 or transmitting it to others.
This fact has been well known since before the start of the pandemic. Even more evidence was produced and readily available by the summer of 2020.
The face mask has become the international symbol of Covid-19 and for those who have not studied the issue, remains an important method to protect themselves and others.
Sadly, they could not be more wrong or ill-informed.
I blame government officials in collaboration with big tech, mainstream media and social media for amplifying and spreading falsehoods that have resulted in countless injuries and even death due to policies forced on the public.
It’s time to shine a bright light of truth on this and many other issues that have served only to harm the public, punish people without due cause and restrict liberties and freedoms worldwide.



